WUNRN
Health and Human Rights Journal 2014, 16/1
ISRAEL – DEPRESSIVE SYMPTOMS AMONG ARAB BEDOUIN WOMEN WHOSE HOUSES
ARE UNDER THREAT OF DEMOLITION IN SOUTHERN ISRAEL: A RIGHT TO HOUSING ISSUE
Nihaya Daoud and Yousef Jabareen
Abstract
Housing is a fundamental human right and a social determinant of
health. According to international law, indigenous peoples are entitled to
special housing and health rights and protections. In Israel, land disputes
between the government and Arab Bedouins, an indigenous minority, have resulted
in ongoing demolitions of Arab Bedouin homes, with thousands more homes
threatened. While demolitions could expose this population to mental health
problems, research linking house demolition and health is scarce. In
this paper, we draw on a human rights perspective to describe this housing
instability and examine the association between the threat of house demolition
and depressive symptoms (DS) among 464 Arab Bedouin women. We conclude
that having their house under threat of demolition is an important determinant
of poor mental health among Bedouin women. Any efforts to decrease DS among
these women will have to take place alongside efforts to stop this practice.
Introduction
Housing is a fundamental human right and a major social
determinant of health.1 The World Health Organization (WHO) has
deemed housing a preexisting condition of health.2 Given the
importance of housing and recognizing their relative disadvantage, minorities
and indigenous peoples are entitled to a special set of health and housing
rights and protections under international law.3 In Israel, land
disputes between successive governments and economically disadvantaged
indigenous Arab Bedouin citizens have resulted in hundreds of house demolitions
every year. Furthermore, thousands of other structures (houses and other
buildings) are under threat of demolition.4 The government
does not recognize Arab Bedouin ownership of many lands, does not allow Arab
Bedouins to erect new structures on what are deemed state lands, and demolishes
structures erected without official permits. Demolitions have increased
dramatically over the past decade. In 2001, 45 homes were taken down in
villages not legally recognized by the Israeli government.5 In 2011 there
were more than 1000 demolitions, with thousands more structures currently at
risk.6
The association between house demolition and mental health has
received little attention. However, previous studies have linked displacement
and relocation due to political conflict with high psychological distress and
adverse mental health.7 In this paper, we first adopt a human
rights lens to describe demolitions in Arab Bedouin communities in Israel. We
then draw on place attachment theory to discuss the link between living in a
house under threat of demolition and depressive symptoms among Bedouin women.
The rights of minorities and indigenous groups to health and
housing
The Universal Declaration of Human Rights (UDHR) serves as the basis for human
rights legal instruments. Article 25 links housing to health: “Everyone has the
right to a standard of living adequate for the health and well-being of himself
and of his family, including food, clothing, housing, medical care and
necessary social services…”8 Minorities and indigenous peoples enjoy
a special set of rights and protections as laid out in the Declaration on the
Rights of Persons Belonging to National or Ethnic, Religious and Linguistic
Minorities, adopted in 1992. This was the first international document
dedicated solely to minority rights. General Comment 4 to the International
Covenant on Civil and Political Rights (ICCPR), adopted in 1966, addresses
issues frequently encountered by minorities and disadvantaged groups, including
the need to protect their rights to housing and health.9
Recognizing the unique disadvantage faced by indigenous groups,
the international community later developed an additional document addressing
the needs and group-defining characteristics of these peoples.10 The Declaration
on the Rights of Indigenous Peoples, adopted in 2007, outlines key collective
rights, such as self-determination and land rights.11 Article 21.1
specifies the rights relevant to this paper: “[i]ndigenous peoples have the
right, without discrimination, to the improvement of their economic and social
conditions, including, inter alia, in the areas of education, employment,
vocational training and retraining, housing, sanitation, health and social
security.” Building on these basic rights, Article 23 states that “[i]ndigenous
peoples have the right to determine and develop priorities and strategies for
exercising their right to development. In particular, indigenous peoples have
the right to be actively involved in developing and determining health, housing
and other economic and social programs affecting them and, as far as possible,
to administer such programs through their own institutions.” This Article
emphasizes the right of indigenous groups to participate in determining their
housing situation.
Specifically in relation to health, Article 24.2 declares that “[i]ndigenous
individuals have an equal right to the enjoyment of the highest attainable
standard of physical and mental health. States shall take the necessary steps
with a view to achieving progressively the full realization of this right.” Together,
these Articles create a basis for understanding the special housing and health
rights granted to indigenous peoples.
The right to housing is integrally related to the right to land.
Importantly, the 2007 Declaration also addresses indigenous land rights—a
particularly contentious issue. Article 27 of the Declaration outlines
obligations in relation to these rights, while Article 28 confirms the right of
indigenous peoples “(1) [t]o redress, which can include restitution or, when
this is not possible, just, fair and equitable compensation, for the lands,
territories and resources which they have traditionally owned or otherwise
occupied or used, and which have been confiscated, taken, occupied, used or
damaged without their free, prior and informed consent.” It also states that “(2)
[u]nless otherwise freely agreed upon by the peoples concerned, compensation
shall take the form of lands, territories and resources equal in quality, size
and legal status or of monetary compensation or other appropriate
redress.” Therefore, not only are the basic rights to housing and health
guaranteed; the Declaration goes much further by recognizing the land rights of
indigenous peoples and outlining state obligations in this regard.
The land, housing, and health rights detailed in the Declaration
on the Rights of Indigenous Peoples are relevant to Arab Bedouins in Israel,
who are an indigenous minority. Below, we examine demolition of Arab Bedouin
houses by the Israeli governments in relation to these rights.
The right to housing and health: The case of the Arab Bedouins in
the Negev
The Arab Bedouins have lived in the Negev (Naqab), now part of Israel’s
southern region, since long before the establishment of the state of Israel in
1948.12 The Arab Bedouins, who number about 200,000, are now
Arab-minority citizens of Israel. They make up about 25% of the population of
the Negev, yet they have jurisdiction over less than 3% of the land.13 Arab Bedouins
are also among the poorest and most disadvantaged groups in Israel.14
Although the Arab Bedouins are indigenous to the region, not all
of their current towns and villages predate Israel’s establishment. Seven
townships and villages were established in the early 1950s and 1960s following
forced population evictions and transfers to a specific part of Negev called
the Siyag (Arabic for fence).15 During this period, the Israeli
government sought to concentrate Arab Bedouins in the Siyag, informing them
that the transfer was temporary; however, they were never allowed to return to
their lands.16 While about half of the Arab Bedouin population moved to
these seven new villages, the other half remained in about 47 villages. The
Israeli government did not legally recognize these original villages, and
today, Israeli authorities consider the Arab Bedouins residing in these
villages to be squatters on state land. In 1965, Israel enacted the Planning
and Building Law, followed by a national building master plan. Though Arab
Bedouin villages predate this process, they were not recognized in official
state documents or legislation. According to the Planning and Building Law,
structures built in these communities are illegal and the settlements are
deemed “unrecognized.” As such, state authorities refuse to provide people
living in these areas with infrastructure, depriving them of connections to
national electrical and telecommunications grids, water and sewage systems, and
paved roads.17 The unrecognized villages also lack education, welfare, health,
and employment services.18 Despite these conditions, Arab Bedouins
continue to reside there. They are reluctant to leave because of their
historical, cultural, and emotional connections to the land, and because they
know their departure would result in land loss. Thus, about half of the Arab
Bedouins – some 90,000 people – now live in shacks and other temporary
dwellings without access to basic infrastructure.19
The Israeli government has attempted to deal with land claims from
the Arab Bedouins, but the state’s plans fail to recognize the basic land
rights of the Arab Bedouins and conflict with the express desires of the
community.20 In fact, due to a history of broken promises, lack of
follow-through, and inconsistent policy, the Arab Bedouins do not consider the
government a credible partner.21 Consequently, the problem of the
unrecognized villages remains unresolved.
In the absence of official planning, and because Arab Bedouins are
unable to gain legal recognition and ownership of their lands, construction in
unrecognized villages is carried out without permits. According to a report by
Human Rights Watch, in recent years most Arab Bedouins have given up appealing
house demolition orders in court, because Israeli judges have historically
failed to nullify demolition orders in unrecognized villages.22 As a result,
residents live with the constant knowledge that their homes might be destroyed.
This is a tangible threat; since the 1970s, there have been thousands of such
demolitions, though accurate numbers have not been published by the Israeli
authorities.23 In one village, Al-Aarkib, houses have been demolished more than
65 times since 2010; the villagers rebuilt after each demolition.24
Study methodology
Our study postulates that the frequency of house demolitions, and living with
the constant threat of demolition, might expose the entire Arab Bedouin
community to poor mental health. Women may be particularly impacted since they
are a more vulnerable group in this community: Arab Bedouin women act as the
main caregivers in their families, and a constant threat of house demolition
might elevate stress due to the jeopardy this places their children in, leading
to detrimental mental health effects.25 Drawing on place attachment
theory, research has shown direct associations between detachment from place,
displacement due to conflict, and political violence, and adverse mental health
effects and psychological distress.26 For example, long-term
trauma-related illnesses were found among displaced Vietnamese refugees in
Australia, and forced displacements in World War II were associated with mental
health disorders and poor quality of life among elderly persons in Germany.27 Palestinian
Arabs who were internally displaced from their lands and homes following the
establishment of the state of Israel suffered from poorer self-rated health and
higher chronic illnesses compared to non-displaced persons.28 There might also
be indirect associations between displacement and poor mental health, and low
socioeconomic position of displaced persons.29 Research shows
that displaced persons tend to live in poor housing conditions and to have low
income, since they lose all of their belongings and social standing when they
are displaced.30 While not all Arab Bedouins in Israel have been displaced, this
study addresses whether the ongoing threat of demolition contributes to poor
mental health in the same way that physical displacement does.
While we hypothesize a direct association between housing
instability and depressive symptoms (DS) among Arab Bedouin women living in
southern Israel, we also acknowledge the possibility of an indirect association
mediated by women’s socioeconomic positions and the physical features of their
houses. Living in unrecognized villages might be another factor in DS, as these
villages lack basic infrastructure and access to proper health and education
services. To examine the contribution of houses under threat of demolition to
DS, we first examined the direct associations between these variables.
Employing different multivariable models, we then took into consideration the
women’s socioeconomic position (education, income, and literacy), as well as
physical features of their houses (type of building, connection to water and
electricity, house crowding, and access to public of transportation) and the
location of the house (in legally recognized and unrecognized localities).
Method
Sample and data collection
Data for the study were obtained from a cross-sectional survey of Arab Bedouin
women aged 18-49 years. Between July 2008 and January 2009, trained
female interviewers approached all 1,175 women who visited 14 Mother and Child
Health (MCH) clinics in southern Israel. Eligible women (n=540) who had given
birth to a full-term baby and whose child was 9-15 months age at the time were
asked to participate in the study. Women who agreed (n=464) were interviewed
using a structured, Arabic-language questionnaire after signing an informed
consent form. The response rate was 86%. The study was approved by the
Institutional Ethics Committee of the Soroka University Medical Center.
Measures
We measured DS using the Center for Epidemiologic Studies Depression Scale
(CES-D) short form, which includes seven item-screening questions on DS
experienced in the past week.31 This scale has been translated
and validated in Arab populations.32 The internal consistency of the
scale in the Arab population in Israel was 0.86, and in the current study. The
internal consistency of the scale measured by Cronbach’s alpha was 0.805.33 The mean score
of DS was 7.11 (SD=.54), the median score was six, and range was zero to 21. We
dichotomized DS into two groups using the median as the cutoff point: low DS
(zero to six symptoms per week) and high DS (more than six symptoms per week).
We then measured the independent variable of having a house under
threat of demolition using participants’ answer to the question: Is your house
designated for demolition? (Answer categories: yes or no.)
We determined women’s socioeconomic position by three measures:
- a) Women’s education: the highest level of education
the woman had achieved. We grouped responses into two categories: (1) less
than high school and (2) high school and above.
- b) Family source of income: whether the family’s main
income came from work or social security allowances. A family is eligible
for social security allowances if they are unemployed or their income is
less than the minimum wage.
- c) Ability to read and write in Arabic: whether the
participant had the ability or not to read and write in her mother tongue
(Arabic).
We assessed physical features of the house using women’s answers
to six questions:
- Type of building: whether the house is (1) a temporary
structure, such as a tent (which is less stable housing), or (2) a
permanent building.
- House crowding: derived from other variables by
dividing the total number of persons living in one household by the number
of rooms in the house. This revealed a continuous variable that was dichotomized
into less-crowded houses (with one or two persons per room) and high
degree of crowding (with three to 12 persons per room).
- House connected to electricity: Answer categories were
(1) yes, always connected, and (2) no, not connected, or not always
connected.
- House connected to water supply: Answer categories were
(1) yes, always connected and (2) no, not connected or not always
connected.
- House in a village with access to public
transportation: Answer categories were (1) yes and (2) no.
- House location: whether the house was located in a
legally recognized or unrecognized village. Answer categories were (1) yes
and (2) no.
Statistical analysis
We first conducted univariate analysis for the associations between independent
variables and house under threat of demolition. We then used multivariable
logistic regression analysis to examine the association between house under
threat of demolition and DS in different models, while adjusting for groups of
independent variables. The multivariable models were as follows: model 1 was
unadjusted, model 2 was adjusted for the women’s SEP (women’s education, family
source of income, and literacy), model 3 was adjusted for women’s SEP and the
physical features of the house (type of building, connection to water and
electricity, house crowding, and house in a village with access to public
transportation), and the final model (model 4) was adjusted for all of the
variables in model 3, in addition to the location of the house (in legally
recognized versus unrecognized village). Variables in the models were
considered significant at the level of 5% (p-value).
Results
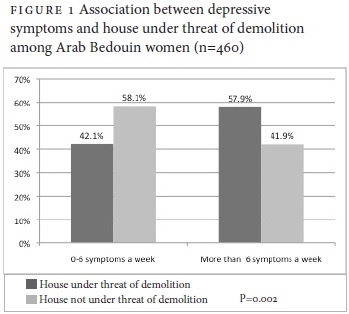
27.2% of the study participants reported that their house is under
threat of demolition. Women living in a house under threat of demolition had
significantly higher DS (more than six symptoms a week) compared to women who
do not live in such a house; 57.9% and 41.9%, respectively (Figure 1).
Women living in a house under threat of demolition had poorer SEP
compared to those in stable housing (Table 1); 68% of these women had fewer
than 12 years education compared to 44.6% in the other group; half of their
families relied on social security allowances as their main source of income, compared
to 35.3% among women whose houses were not under threat of demolition; and
close to 42% were not able to read and write, compared to 15% of the women not
living in a house under threat of demolition.
Eighty five percent of the women living under threat of demolition
also lived in poor housing conditions, while only 15% of women whose homes were
not under threat of demolition lived in poor conditions. Sixty four percent of
the women who lived in a house under threat of demolition reported that their
house was not connected to the electrical grid (never or inconsistently),
compared to 22.4% of women not under this threat. Seventy four percent of women
living in a house under threat of demolition reported that their house was not
connected to a water supply, compared to only 2.4% of women in houses not under
this threat. House crowding was greater in houses under threat of demolition
(58.7% vs 34.8%). About 70% of the houses under threat of demolition are
located in villages that lack public transportation, and 76.2% of the houses
under threat of demolition were in unrecognized villages.


The multivariate logistic regression results revealed a robust
association between house under threat of demolition and DS among Arab Bedouin
women, even after accounting for the women’s SEP, the physical features of the
house, and the house location in legally recognized or unrecognized villages
(Table 2). The unadjusted model (Model 1) showed that women who live in a house
under threat of demolition had significantly (P<0.003) higher DS (Odds Ratio
(OR)=1.92, 95% confidence interval (CI)=1.25-2.96). The magnitude (OR) of this
association was almost unchanged in all the following models; that is, after
adjusting for women’s SEP in Model 2 (OR= 1.88, 95%CI=1.18-2.98), accounting
for the physical features of the house in Model 3 (OR=1.96, 95%CI=1.04-3.70),
and in Model 4 when adjusting for house location in addition to all the other
variables (OR=1.99, 95%CI=1.03-3.82).
Notably, women’s SEP (education, family source of income, and
ability to read and write) remained significant in all adjusted models.
However, the variables related to physical features of the house and the house
location were not significant in Models 3 and 4.

Discussion
The context of this study is complex and includes legal and
political aspects rooted in Israel’s refusal to recognize the land rights of
the Arab Bedouin indigenous minority. The human rights perspective we adopt
provides a suitable framework to describe this complexity. According to
Abu-Rabia and others, house demolitions amount to a violation of the basic
human right to housing and living with dignity, as well as other rights, such
as that of self-determination.34
Official organs of the Israeli government currently do not regard
the Arab Bedouin as an indigenous minority, although the international
community does.35 Historians agree that the Arab Bedouins have inhabited the Negev
since the seventh century and were the only inhabitants of the desert until the
mid-twentieth century. Most of the Negev Bedouin are related to Sinai and
Arabian Peninsula Bedouin tribes. While the Bedouin were traditionally a
nomadic people who raised livestock through grazing, they adopted a largely
sedentary way of life prior to the establishment of the state of Israel in
1948. Accordingly, they settled in distinct villages with well-defined and
traditional systems of communal and individual land ownership.36 Indeed, the way
of life and difficulties the Arab Bedouin face in maintaining their cultural
identity and connections to their traditional lands have been similar to the
problems faced by indigenous peoples worldwide.37 The Committee on
the Elimination of Racial Discrimination (CERD) has also addressed this issue.38 In June
2007, CERD recommended that the Israeli government officially recognizes the
unrecognized villages and, in the event that they refuse, that they consult the
residents before any further relocations.39 In 2012, CERD
expressed its concerns about the housing and planning conditions of the Arab
Bedouin community.40 The UN Human Rights Committee (HRC) highlighted allegations of
forced evictions of Arab Bedouins and referred to the inadequate consideration
of Arab Bedouins’ needs.41
Despite the condemnation by UN monitoring committees, and assorted
plans initiated over the years, Israel’s policy toward the Arab Bedouin citizens
and their unrecognized villages remains largely unchanged. For example, while
the 2008 Goldberg Commission called on the government to “recognize as many
villages as possible,” in 2012 the government temporarily embraced a different
proposal, the Prawer Plan. The Prawer Plan (put forth in September 2011) would
have forcibly evacuated and transferred over 40,000 citizens from their
villages and concentrated them in planned towns.42 It failed to
recognize the rights of some 70,000 Arab Bedouins in unrecognized villages and
denied them their status and rights as an indigenous minority, despite their
historical ties to the land. This is in direct conflict with the Declaration of
the Rights of Indigenous Peoples.43 The Prawer Plan was greeted
with both international and local opposition, and was withdrawn in December
2013.44
Our findings suggest that in the case of Arab Bedouin women in
Israel, threat of housing demolition creates higher DS, even after adjusting
for women’s SEP, physical features of the house, and house location. Previous
studies have shown that the actual act of displacement or of losing a house is
associated with poor mental health.45 In the current study, we
show that the threat of displacement alone is enough to create DS.
The strength of the association between house under threat of
demolition and DS can be viewed through the lens of place attachment theory,
which has examined the connection between place and health.46 While our study
sample had not all been displaced, we suggest they may as well have been, since
the threat of house demolition severed their secure connection to place.47 The place
attachment theory presupposes that people have attachments to the places they
inhabit and that they develop and maintain spatial identity based on their
experiences with particular places. For indigenous people, prolonged
residence in one place and attachment to their land are significant elements of
collective identities.48 When this spatial identity is
interrupted by conflict or forced displacement, communities can become
dysfunctional, and this can have serious impacts, including psychological
disruption.49 Health research has shown that being forcibly displaced is
trauma-inducing.50 Such displacement has been related to both short- and long-term mental
illness.52 Forced displacement and threat of home loss may prompt fear of
identity loss, and might be related to high stress levels and post-trauma. A
small qualitative study among Arab Bedouin children in the Negev and a study on
internal displacement among Palestinian Arabs in Israel found high levels of
stress among those who had been displaced, which may be correlated with mental
illness. While we did not measure stress levels in the current study, we
pose that this finding might be an important area of study for future research
with this community.
While Brown and Perkins argue that communities experiencing
displacement subsequently undergo a coping phase during which they develop an
attachment to their new location, we postulate this is not the case in our
study, as the threat of demolition is both real and open-ended; there are no
immediate alternative homes available, and Arab Bedouins, unable to rely on
their current dwelling, do not have the privilege of coping and developing an
attachment to a new place.53 Many families are left homeless after
their house is demolished. Under the Building and Planning Law, villagers are
not entitled to alternative shelter—temporary or permanent—nor are they
compensated for their losses.54 After suffering the
psychological and financial losses that accompany destruction of their
residence, many people revert to living in tents and other impermanent
structures to prevent repeat demolition and further trauma. Although other
villagers may help them to rebuild, the new house is, once again, under
constant threat of demolition. This might be another source of stress in this
community.
Human Rights Watch reports have outlined other factors that can
elevate stress and expose Arab Bedouin women and the entire Arab Bedouin
community to depression. For example, it has been reported that there is often
no advance warning of demolitions, and consequently families cannot prepare for
them.55 In addition, while in the past Israeli authorities destroyed a
few structures at a time, they have increasingly carried out mass demolitions,
targeting entire neighborhoods or villages.56 Some
villages have been destroyed many times.57 Advanced warning
of a demolition is sometimes used as a pressure tactic; the demolitions are not
necessarily carried out. Conversely, in most cases, as there is no warning, the
community lives with fear of the unknown, which we speculate would generate tremendous
stress and could increase mental health concerns.58 Furthermore, the
process of issuing warnings and carrying out demolitions is often accompanied
by violence. When issuing demolition orders, it is common for law-enforcement
officials to appear in a large show of force. Meanwhile, villagers attempt to
physically impede the demolitions.59 At times, residents are able to
salvage some of their belongings; in other cases, their personal property is
destroyed or confiscated. To prevent the loss of their belongings, some
villagers destroy their homes with their own hands, an action that again we
speculate would elevate stress and expose them to adverse mental health
effects.60
The association between house under threat of demolition and DS
might also relate to the social determinants of health in the displaced
populations acting as mediating factors. Displaced persons tend to experience
unstable housing and live in poor housing conditions, due to their relative
poor SEP and low income.61 Emerging health research has found that
poor quality or substandard housing (dampness, mold, overcrowding, lack of safe
drinking water and hot water, etc.) and financial insecurity are linked to poor
physical health and to psychological distress.62 While in this
study poor physical features of the house (type of building, house crowding,
house connection to water supply and electricity, and house access to public
transportation) were higher in houses under threat of demolition, this factor
was not significant in explaining DS in the multivariate models. A possible
explanation could be that most of the Arab Bedouin population lives in poor
housing conditions and poverty; it is the unstable housing situation that
creates high levels of stress, especially for women. In a Human Rights Watch
study, women whose houses were demolished stated that they did not have a room
in which to bathe their children or store their belongings.63 In a
previous focus group study, Arab Bedouin women mentioned that their living
conditions and the threat of house demolition were major obstacles to infant
care and were a source of stress.64
Our finding that women’s SEP was significant even after adjusting
for housing features indicates the importance of these variables in explaining
DS among Arab Bedouin women. Generally, Arab Bedouin women have low SEP.65 Our results
reveal that women whose houses are under threat of demolition have poorer SEP
compared to those whose houses are not under such threat. In all likelihood,
the granting of full rights to access health care, education, and employment,
as outlined in various human rights instruments, would improve these women’s
SEP, improve their health, and help to reduce DS among them. However, it cannot
eliminate the adverse effects of having a house under threat of demolition on
their DS.
Interviewing women who visit MCH clinics may have created a
selection bias, since more women from recognized villages and towns visit the
MCH clinics than from unrecognized villages, while house demolitions occur more
frequently in the unrecognized villages. However, the demographic distribution
of our study variables shows that the education, family sources of income, and
ability to read and write of our participants are similar to those of Arab
Bedouin women in southern Israel in general. While our study found that having
a house under threat of demolition is linked with higher DS among Arab Bedouin
women, future studies could examine other adverse psychological effects of
actual demolition, including post-trauma, stress, anxiety, and other mental
health problems.
Conclusion
The current study demonstrates that the threat of house demolition
is associated with higher DS among Arab Bedouin women. The Arab Bedouins are an
indigenous minority entitled to housing and health rights, as specified in
various international legal human rights instruments, including those ratified
by Israel. Until the Israeli government respects the rights of its indigenous
people to housing, and stops house demolitions and threats of house
demolitions, Arab Bedouins will remain exposed to increased depressive
symptoms.
Nihaya Daoud, MPH, PhD, is a lecturer at the Faculty
of Health Science, Ben-Gurion University, Beer Sheva, Israel.
Yousef Jabareen, SJD, is a lecturer at Tel-Hai College
and the University of Haifa, Haifa, Israel.
References
1. Commission on Social Determinants of Health, Closing the gap
in a generation: Health equity through action on the social determinants of
health (Geneva: World Health Organization, 2008). Available at http://whqlibdoc.who.int/publications/2008/9789241563703_eng.pdf.
2. World Health Organization, The Ottawa Charter for Health
Promotion (Ottawa, Ont.: World Health Organization, 1986). Available at http://www.who.int/healthpromotion/conferences/previous/ottawa/en/.
3. United Nations Human Rights Council, Report by the Special
Rapporteur on the rights of indigenous peoples, UN Doc. No. A/HRC/18/35/ADD.1
(2011). Available at
http://www.ohchr.org/documents/issues/ipeoples/sr/a-hrc-18-35-add-1_en.Pdf.
4. J. Zayyadna, Report on house demolitions of Arab Bedouins in
the Negev (Be’er Sheva, Israel: Negev Coexistence Forum for Civil Equality,
2012). Available at http://www.Dukium.Org/eng/wp-content/uploads/2011/06/dukiumhousedemoeng1.pdf.
5. C. Noah, A report on house demolitions of Arab Bedouins in
the Negev (Hebrew) (Be’er Sheva, Israel: Negev Coexistence Forum for Civil
Equality, 2011). Available at http://www.dukium.org/heb/wp-content/uploads/2012/03/demolitions_report_2011-heb-with-summry.pdf.
6. Zayyadna (see note 4).
7. N. Daoud, K. Shankardass, P. O’Campo, et al., “Internal
displacement and health among the Palestinian minority in Israel,” Social
Science and Medicine 74/8 (2012), pp. 1163-1171; D. Pedersen, “Political
violence, ethnic conflict, and contemporary wars: Broad implications for health
and social wellbeing,” Social Science & Medicine 55/1 (2002), pp.
175-190; P. Spiegel, F. Checchi, S. Colombo, E. Paik, “Health-care needs of
people affected by conflict: Future trends and changing frameworks,” Lancet
375/9711 (2010), pp. 341-345; Z. Steel, D. Silove, T. Phan, A. Bauman, “Long-term
effect of psychological trauma on the mental health of Vietnamese refugees
resettled in Australia: A population-based study,” Lancet 360/9339
(2002), pp. 1056-1062.
8. Universal Declaration of Human Rights (UDHR), G.A. Res. 217A
(III) (1948), Art. 71. Available at http://www.un.org/Overview/rights.html.
9. International Covenant on Civil and Political Rights (ICCPR),
G.A. Res. 2200A (XXI) (1966). Available at http://www.ohchr.org/EN/ProfessionalInterest/Pages/CESCR.aspx.
10. Declaration on the Rights of Indigenous Peoples, G.A. Res.
61/295 (2007). Available at http://www.un.org/esa/socdev/unpfii/documents/DRIPS_en.pdf.
11. T.Y. Jabareen, “Redefining minority rights: Successes and
shortcomings of the UN Declaration on the Rights of Indigenous Peoples,” UC
Davis Journal of International Law and Policy 18 (2012), pp. 119-161.
12. I. Abu-Saad, “Introduction: State rule and indigenous
resistance among al naqab Bedouin Arabs,” Hagar: Studies in Culture, Polity
and Identities 8/2 (2008), pp. 2-24.
13. Zayyadna (see note 4); T. Abu-Ras, Land disputes in Israel:
The case of the Bedouin of the Naqab (Adalah Newsletter, April 2006).
Available at http://www.adalah.org/newsletter/eng/apr06/ar2.pdf.
14. S. Abu-Bader and D. Gottlieb, Poverty, education and
employment in the Arab-Bedouin society: A comparative view (Jerusalem:
National Insurance Institute, 2012). Available at http://www.btl.gov.il/Publications/research/Documents/mechkar_98.pdf.
15. Abu-Saad (see note 12).
16. S. Swirsky and Y. Hasson, Transparent citizens: Government
policy toward the Bedouin in the Negev, (Tel Aviv, Israel: ADVA Center,
2005). Available at http://www.adva.org/uploaded/NegevEnglishSummary.pdf.
17. Abu-Saad (see note 12).
18. W. Abbas, The bare minimum – health services in the
unrecognized villages in the Negev (Jaffa, Israel: Physicians for Human
Rights – Israel, 2009). Available at http://www.phr.org.il/uploaded/phr%20-%20bare%20minimum%20-%20health%20services%20in%20the%20unrecognized%20villages%20(3).pdf.
19. Human Rights Watch, Off the map: Land and housing rights
violations in Israel’s unrecognized Bedouin villages (Human Rights Watch,
2008.) Available at http://www.hrw.org/reports/2008/iopt0308/iopt0308web.pdf.
20. O. Yiftachel, “Bedouin-Arabs and the Israeli settler state:
Land policies and indigenous resistance,” in D. Champange and I. Abu-Saad
(eds), The future of indigenous peoples: Strategies for survival and
development (Los Angeles, CA: UCLA American Indian Studies Center, 2003),
pp. 21-47.
21. R. Aburabia, Principles for arranging recognition of the
Bedouin villages in the Negev: Position paper (ACRI, Bimkom and PCUV,
2011). Available at http://www.acri.org.il/en/wp-content/uploads/2011/09/Prawer-Policy-Paper-May2011.pdf.
22. Human Rights Watch (see note 19).
23. Aburabia (see note 21), R. Aburabia, Principles for
arranging recognition of the Bedouin villages in the Negev: Policy brief (ACRI,
Bimkom and PCUV, 2011). Available at http://www.acri.org.il/en/wp-content/uploads/2011/09/Prawer-Policy-Brief-FINAL-ENG.pdf;
Human Rights Watch (see note 19).
24. Zayyadna (see note 4).
25. N. Daoud , I. Shoham-Vardi , LM. Urquia, P. O’Campo, “Polygamy
and poor mental health among Arab Bedouin women: Do socioeconomic position and
social support matter?” Ethnicity & Health 19/4 (2014), pp. 385-405;
Human Rights Watch (see note 19).
26. D. Stokols, S. Shumaker, J. Martinez, “Residential mobility
and personal well-being,” Journal of Environmental Psychology 3/1
(1983), pp. 5-19; Daoud (2007, see note 7); M.V. Giuliani and R. Feldman, “Place
attachment in a developmental and cultural context,” Journal of
Environmental Psychology 13/1 (1993), pp. 267-274.
27. Steel (see note 7); S. Freitag, E. Braehler, S. Schmidt, H.
Glaesmer, “The impact of forced displacement in World War II on mental health
disorders and health-related quality of life in late life – a German
population-based study,” International Psychogeriatrics 25/2 (2013), pp.
310-319.
28. Daoud (2012, see note 7).
29. Ibid.
30. Ibid.; K.E. Miller and A. Rasmussen, “War exposure, daily
stressors and mental health in conflict and post-conflict settings: Bridging
the divide between trauma-focused and psychosocial framework,” Social
Science & Medicine 70/(2010), pp. 7-16.
31. L. Radloff, “The CES-D scale: A self-report depression scale
for research in the general population,” Applied Psychological Measurement
1/3 (1977), pp. 385-401.
32. R. Ghubash, T. Daradkeh, K. Naseri, et al., “The performance
of the center for epidemiologic study depression scale (ces-d) in an Arab
female community,” International Journal of Social Psychiatry 46/4
(2000), pp. 241-249.
33. N. Daoud, V. Soskolne, O. Manor, “Educational inequalities in
self-rated health within the Arab minority in Israel: Explanatory factors,” European
Journal of Public Health 19/5 (2009), pp. 477-483.
34. Abu Rabia (2011, see note 21); Human Rights Watch (see note
19).
35. H. Yahel, R. Kark, S.J. Frantzman, “Are the Negev Bedouin an
indigenous people? Fabricating Palestinian history,” Middle East Quarterly
Summer (2012), pp. 3-14; Adalah – The Legal Center for Arab Minority Rights
in Israel, The Arab Bedouin of the Naqab: Myths and misconceptions (Haifa:
Adalah, 2013). Available at http://adalah.org/images/mythsflyerweb.pdf;
United Nations Human Rights Council (see note 3).
36. Yiftachel (see note 20).
37. United Nations Human Rights Council (see note 3).
38. UN Committee on the Elimination of Racial Discrimination,
Report on the Seventieth session (19 February-9 March 2007) and Seventy-first
session (30 July-17 August 2007), UN Doc. No. A/62/18, (2007) para. 218.
Available at http://www.refworld.org/docid/473424062.html
(2007).
39. Ibid.
40. UN Committee on the Elimination of Racial Discrimination,
Consideration of reports submitted by States parties under Article 9 of the
Convention Concluding Observations of the Committee on the Elimination of
Racial Discrimination, UN Do. No. CERD/C/ISR/CO/14-16 (2012) para. 20.
Available at http://www2.ohchr.org/english/bodies/cerd/docs/cerd.C.Isr.Co.14-16.pdf.
41. UN Human Rights Committee, Consideration of reports submitted
by States parties under Article 40 of the Covenant Concluding observations of
the Human Rights Committee. UN Doc. No. CCPR/C/ISR/CO/3), (2010), para. 24.
Available at http://unispal.un.org/UNISPAL.NSF/0/51410EBD25FCE78F85257770007194A8.
42. T. Dahan, The State of human rights in Israel and in the
Occupied Territories 2012: Situation report (Tel Aviv, Israel: ACRI, 2012).
Available at http://www.acri.org.il/en/2012/12/16/acri-situation-report-2012.
43. United Nations (2007, see note 10).
44. Adalah (see note 35).
45. Steel (see note 7); Daoud (2012, see note 7).
46. I. Altman and S.M. Low, Place attachment. A conceptual
inquiry, (New York, NY, US: Plenum Press, 1992); S. Macintyre, A. Ellaway,
S. Cummins., “Place effects on health: How can we conceptualise, operationalise
and measure them?,” Social Science and Medicine 55/1 (2002), pp. 125-139.
47. Ibid.; M.A. Davenport and D.H. Anderson, “Getting from sense
of place to place-based management: An interpretive investigation of place
meanings and perceptions of landscape change,” Society and Natural Resources
18/7 (2005), pp. 625-641.
48. B. Brown and D. Perkins, “Disruptions in place attachment,” in
I. Altman and S.M. Low, Place attachment. A conceptual inquiry, (New
York, NY, US: Plenum Press, 1992), pp. 279-304.
49. M. Fried, “Continuities and discontiuities of place,” Journal
of Environmental Psychology 20/3 (2000), pp. 193-205; M. Fullilove, “Psychiatric
implications of displacement: Contributions from the psychology of place,” American
Journal of Psychiatry 153/12 (1996), pp. 1516-1523; Steel (see note 7).
50. C. Hartman, “The housing of relocated families,” Journal of
the American Institute of Planner 30/4 (1964), pp. 266-286.
51. Brown and Perkins (see note 48); M. Fullilove (see note 49);
Fried (see note 49); Daoud (2012, see note 7); Yiftachel (see note 20).
52. O. Almi, The ramifications of house demolitions in Israel
on the mental health of children (Tel Aviv, Israel: Physicians for Human
Rights – Israel, 2006). Available at http://www.phr.org.il/uploaded/articlefile_1136475755945.doc;
Daoud (2012, see note 7).
53. Brown and Perkins (see note 48).
54. Aburabia (2011, see note 21); Human Rights Watch (see note
19).
55. Human Rights Watch (see note 19).
56. Aburabia (2011, see note 21); Human Rights Watch (see note
19).
57. Zayyadna (see note 4); Human Rights Watch (see note 19).
58. Aburabia (2011, see note 23).
59. Aburabia (2011, see note 21); Human Rights Watch (see note
19).
60. Ibid.; Ibid.
61. Miller and Rasmussen (see note 30); Daoud (2012, see note 7).
62. M. Shaw, “Housing and public health,” Annual Review of
Public Health 25 (2004), pp. 397-418; J. Krieger and D.L. Higgins, “Housing
and health: Time again for public health action journal information,” American
Journal of Public Health 92/5 (2002), pp. 758-768; G. Evans, N.M. Wells, A.
Moch, “Housing and mental health: A review of the evidence and a methodological
and conceptual critique,” Journal of Social Issues 59/3 (2003 ), pp.
475-500.
63. Human Rights Watch (see note 19).
64. N. Daoud, P. O’Campo, A. Agbaria, et al., “The social ecology
of maternal infant care in socially and economically marginalized community in
Southern Israel,” Health Education Research 27/6 (2012), pp. 1018-1030.
65. Daoud (2014, see note 25).